Minimally Invasive Surgeries
Weight loss surgeries/procedures fall into several different categories. Some surgeries/procedures fall into more than one category. They are as follows:
- Restrictive procedures
- Malabsorptive procedures
- Combination procedures
- Pylorus preserving procedures
- EBTs (Endoscopic Bariatric Therapy)


Restrictive Operations
Purely Restrictive operations have largely been abandoned due to poor weight loss or maintenance of weight loss. Restrictive operations generally work solely by restricting the amount of food someone can eat at one time. They are simpler to do and usually entail sectioning off part of the stomach with either a staple line or belt or band of some sort. There is usually no rearranging of intestine. The best example of a purely restrictive operation is the LapBand. Some would ask “Isn’t the Sleeve gastrectomy purely restrictive?” The answer to that is no. There is restriction in a sleeve however there are other hormonal changes that occur when 70% of the stomach is removed that have a positive effect on metabolism and the sleeve is not interpreted by the body as starvation as is the LapBand. Purely restrictive procedures tend to be interpreted as starvation by the body. Purely restrictive procedures have the least risk for vitamin deficiency.
Malabsorptive Operations
Malabsorptive operations are defined by operations that primarily work by bypassing more than half the small intestine so that there is less absorption of nutrients and calories by the body. This is combined with some sort of milder restriction of the stomach. Though you may think that it is the lack of absorption that is the primary cause of weight loss but it has been shown that it is not simply the malabsorption which results in positive effects. The bypassing of the first part of the small intestine seems to have a very positive metabolic effect on such conditions as diabetes and high cholesterol that can’t be explained by the malabsorption alone. The Biliopancreatic Diversion (BPD) and the Biliopancreatic Diversion with Duodenal Switch (BPD-DS) are the best examples. In both procedures the upper 60% of the small intestine is bypassed (does not see food anymore but is not removed). They differ in how the stomach is reduced in size and whether the pylorus (valve at the end of the stomach) is preserved or not. Malabsorptive operations result in the most weight loss with the highest success at 10 years out from surgery. They also result in the highest risk of vitamin deficiency. There are some out dated misperceptions of malabsorptive operations in that they cause chronic diarrhea and can cause liver failure. When on a balanced diet the chance of chronic diarrhea in a patient that has undergone BPD-DS is approximately 1%. Fatty meals will cause loose stools, however when the person is on a balanced diet, they should have 2-3 soft bowel movements a day. Liver failure was associated with an older malabsorptive procedure that is no longer done, the Jejunoileal bypass, in which 90% of the small intestine was bypassed. Liver failure should not occur with BPD or BPD-DS unless there has been severe noncompliance with diet associated with chronic diarrhea or when there is severe liver disease (near cirrhosis) already present before surgery. In this situation, the intestinal bypassing is reversed.
Combination Procedures
Combination procedures refer to operations in which the stomach is made smaller and less than 50% of the small intestine is bypassed. Gastric Bypass or Roux-en-Y Gastric Bypass (RYGB), is the best example. In a gastric bypass a very small stomach pouch is made from the upper most part of the stomach. The remainder of the stomach and the top 10% of the small intestine is then bypassed. The bottom 90% of the small intestine is then connected to the pouch. Nothing is typically removed and the bottom of the stomach and the upper 10% of the small intestine drain by a connection lower down to join the food. The stomach and upper 10% contain important enzymes and juices that the body needs to properly digest so they are not removed. RYGB is especially good for treating people with Heartburn as there is a 100% success rate with resolving acid reflux after RYGB. The down side of a RYGB is that the pylorus is not part of the food channel anymore and therefore patients can get ulcers right after the pouch if they take in the medications that can cause an ulcer which are called NSAIDs (Nonsteroidal Anti-inflammatory Drugs). NSAIDs include such medications as Aspirin, Motrin, Advil, ibuprofen, Naprosyn, Aleve. Tylenol is not an NSAID, therefore can be taken by patients that choose RYGB. Since the pylorus is not part of the food channel in a RYGB the food is not slowed down as much and RYGB patients are less tolerant to sugars and fats. Sugars and fats in the diet can cause significant discomfort with bloating, cramping, sweating, flushing and this effect is called Dumping Syndrome.
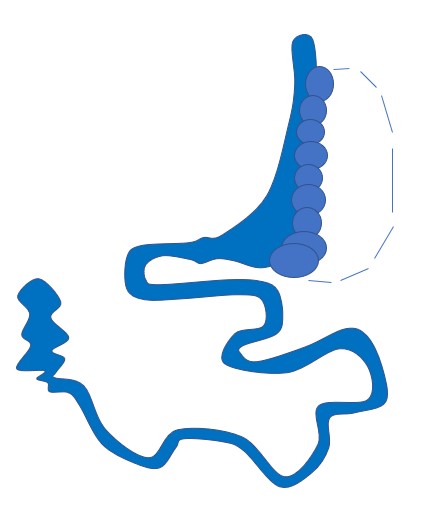
RYGB
Pylorus Preserving Operations
Pylorus preserving operations refer to surgeries in which the valve at the bottom of the stomach, the pylorus, is still part of the food channel. The pylorus has 2 functions. The first is to slow the passage of food from the stomach to the intestine and the second is to protect the intestine right after the stomach from ulcers caused by acid in the stomach. When the pylorus is preserved as is the case with some surgeries, there is less of a chance of ulcer formation and dumping syndrome. People with pylorus preserving surgeries are not restricted from taking NSAIDS. This is helpful to people that need medications for the heart, such as aspirin or medications for the joints, such as ibuprofen. The Gastric Bypass (RYGB) is not a pylorus preserving operation. The following are pylorus preserving operations/procedures, ESG (incisionless sleeve), Sleeve gastrectomy, Switch and Loop Switch.
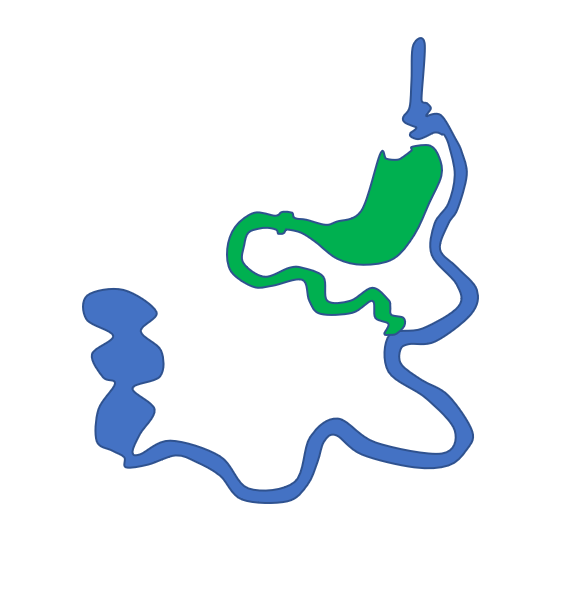
ESG
Endoscopic Sleeve Gastroplasty (No incision)
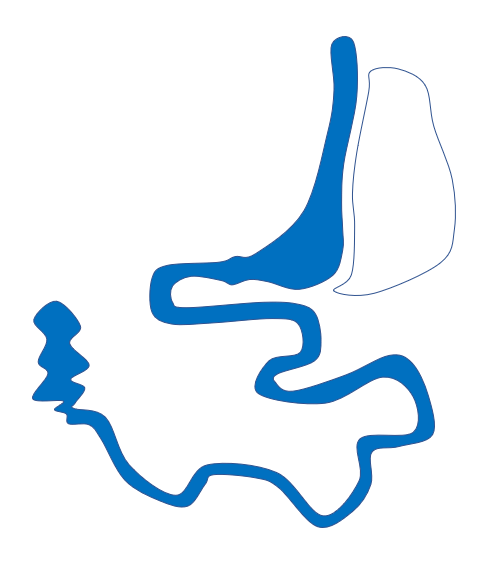
BPD-DS
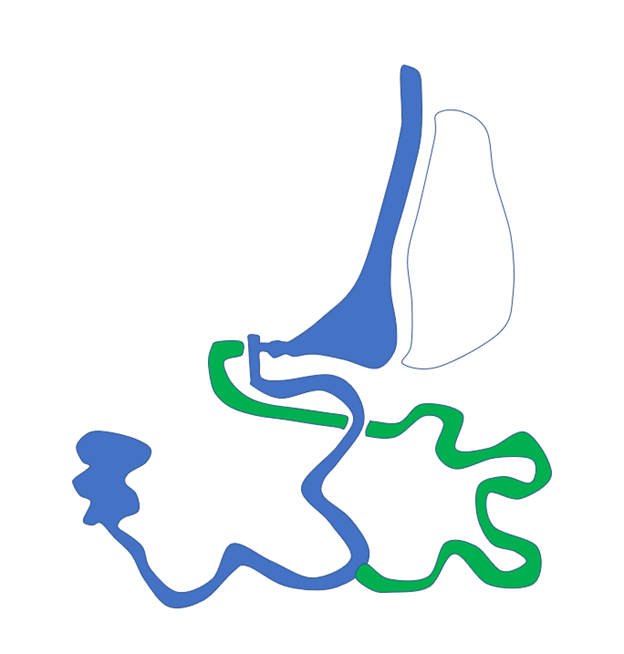
SIPS/SADI
Get In Touch
Call
David Syn, M.D.
President
The Advanced Bariatric Surgery Center, P.A.
Address
3805 22nd Place, Lubbock, TX 79410